Screening children for catecholamine-secreting tumors with a 24-hour urine collection when requesting testing for only vanillylmandelic acid.
Supporting a diagnosis of neuroblastoma
Monitoring patients with a treated neuroblastoma
Clinical Information
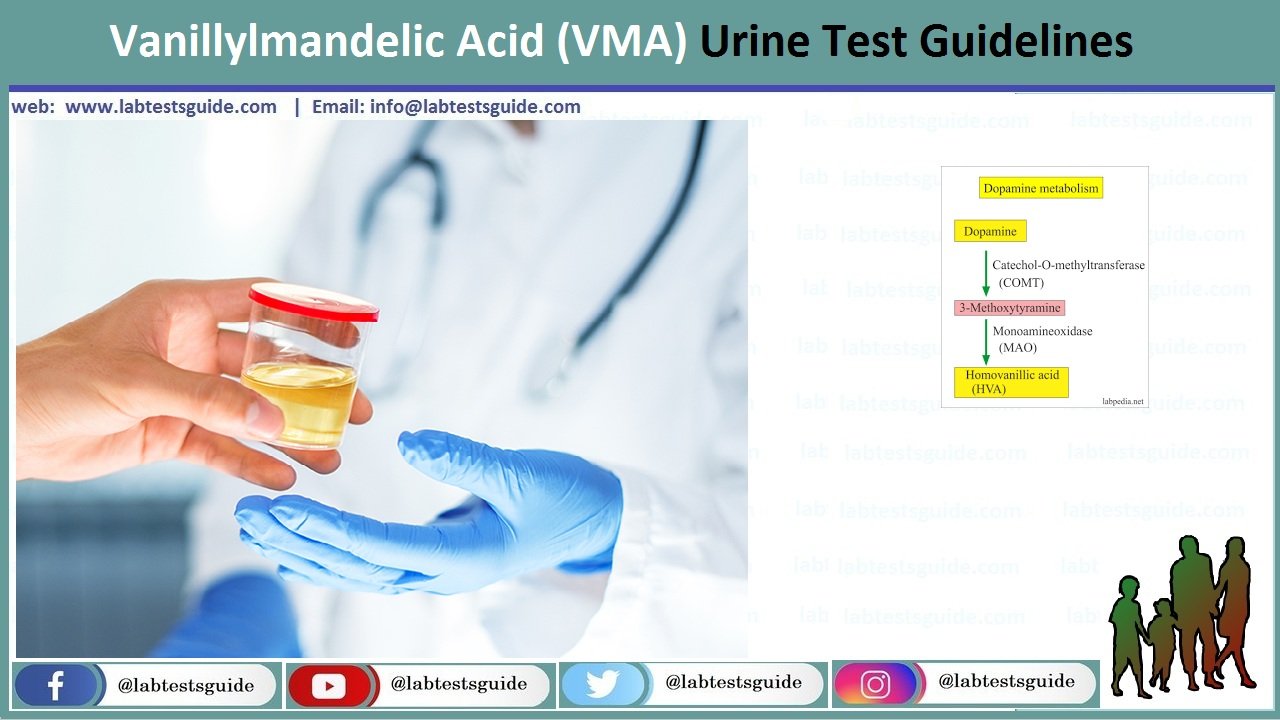
Vanillylmandelic acid (VMA) and other catecholamine metabolites (homovanillic acid [HVA] and dopamine) are typically elevated in patients with catecholamine-secreting tumors (eg, neuroblastoma, pheochromocytoma, and other neural crest tumors). VMA and HVA levels may also be useful in monitoring patients who have been treated as a result of 1 of the above-mentioned tumors.
Why Get Tested?
To help diagnose or rule out a neuroblastoma or other neuroendocrine tumor; to monitor the effectiveness of treatment
Interpretation
Vanillylmandelic acid and/or homovanillic acid concentrations are elevated in most patients (more than 90%) with neuroblastoma; both tests should be performed. A positive test could be due to a genetic or nongenetic condition. Additional confirmatory testing is required.
A normal result does not exclude the presence of a catecholamine-secreting tumor.
Elevated values are suggestive of a pheochromocytoma, but they are not diagnostic.
Cautions
Values are more commonly elevated during a hypertensive episode.
Values may be normal in some individuals with pheochromocytoma.
Sample Required:
- The test is done in the urine.
- Collect 24 hours urine sample.
- Discard the first urine sample and not the time. Now collect all urine samples in the container containing 6 mL of HCl. Collect the last sample when 24 hours are completed.
- Or add 20 mL oh HCL (6mol/L)
- Refrigerate the urine during collection and is stable for 2 weeks.
- The sample is stable for 2 weeks at 2 to 4 °C.
Precautions for Sample:
- Following foods and drugs cause the false raised level of VMA.
- Avoid intake of chocolate, coffee, tea, and cocoa for 2 to 3 days before the test is performed.
- Avoid food like citrus fruits, banana, and food with vanilla.
- Avoid beer and red wine.
- Avoid drugs like aspirin and antihypertensive medicines.
- Vigorous exercise and stress may increase the VMA level.
- Decreased VMA levels may be seen in patients with uremia, alkaline urine, and radiographic contrast media.
- Drugs that may increase the level are levodopa, lithium, nitroglycerine, epinephrine, and caffeine.
- Drugs that may decrease the level are phenothiazine, reserpine, guanethidine, monoamine oxidase inhibitor, and disulfiram.
Normal Values:
Source 1
VMA
| Age | mg/day |
| 0 to 10 day | <1.0 |
| 10 days to 24 months | <2.0 |
| 24 months to 18 years | <5.0 |
| Adult | 2.1 to 7.6 |
Source 2
- Adult/elderly = <6.8 mg/24 hours
- Adolescent = 1 to 5 mg/24 hours
- Child = 1 to 3 mg/24 hours
- Infants = <2 mg/24 hours
- Newborn = <1 mg/24 hours
Other sources
| Test | Urine sample | Plasma |
| VMA | up to 9 mg/24 hours | |
| VMA Some reference says | 2.1 to 7.6 mg/24 hours | |
| Catecholamines total | <100 µg/ 24 hours | |
| Epinephrine | 0 to 20 µg/ 24 hours | <50 pg/mL |
| Metanephrine | 74 to 297 µg/ 24 hours | |
| Norepinephrine | 15 to 80 µg/ 24 hours | 110 to 410 pg/mL |
| Dopamine | 65 to 400 µg/ 24 hours | <87 pg/mL |
Increased VMA Level Is Seen In:
- Adrenal glands tumor (Pheochromocytoma)
- May be seen in any major stress like:
- Burns.
- Body infections ( sepsis).
- Surgery or traumatic injury.
- Many blood pressure drugs.
- Neuroblastoma.
- Ganglioblastoma.
- ganglioneuroma.
- Carcinoid tumors.
Decreased VMA Level Is Seen In:
- In Diabetes
- Parkinsonism.
Increased Catecholamine Is Seen In:
- Pheochromocytoma.
- Neuroblastoma.
- Ganglioneuroma.
- Diabetic acidosis.
- Hypothyroidism.
- Myocardial infarction.
Decreased Catecholamine Is Seen In:
- Parkinsonism.
- Diabetic neuropathy.
Related Articles:
RELATED POSTS
View all