C – reactive protein (CRP) is a native protein synthesized by hepatocytes. It is present in small amounts in normal serum (< 6mg/L). It is named C-reactive protein because it was discovered by its ability to precipitate Pneumococcus C polysaccharide (in 1930). The credit of discovering this acute phase protein goes to Tillett and Francis. The serum level of CRP is raised in response to various inflammatory conditions. Therefore, CRP acts as a marker of inflammation and has a diagnostic significance in determining the disease progression and treatment efficacy. CRP binds to chemical known as phosphocholine which is present in microbes and it help to damage cells and increase phagocytosis by macrophages (monocyte). CRP may also contributes in the clearance of necrotic dead cells and also by apoptotic cells. The acute phase response develops in a wide range of acute and chronic inflammatory conditions like bacterial, viral, or fungal infections; rheumatic and other inflammatory diseases; malignancy; and tissue injury or necrosis. By this action it help to release of interleukin-6 (IL-6) and other cytokines that may aid to trigger the liver to synthesis CRP and fibrinogen proteins. Level of CRP rapidly increase within 2 hours of acute insult, reaching a peak at 48 hours. CRP level fall down after the resolution of acute phase response and have very short life-span of 18 hours. Measuring the CRP level is a screening test for inflammatory diseases and infectious. Rapid, marked increases in CRP occur with inflammation, infection, trauma and tissue necrosis, malignancies, and autoimmune disorders.
PRINCIPLE:
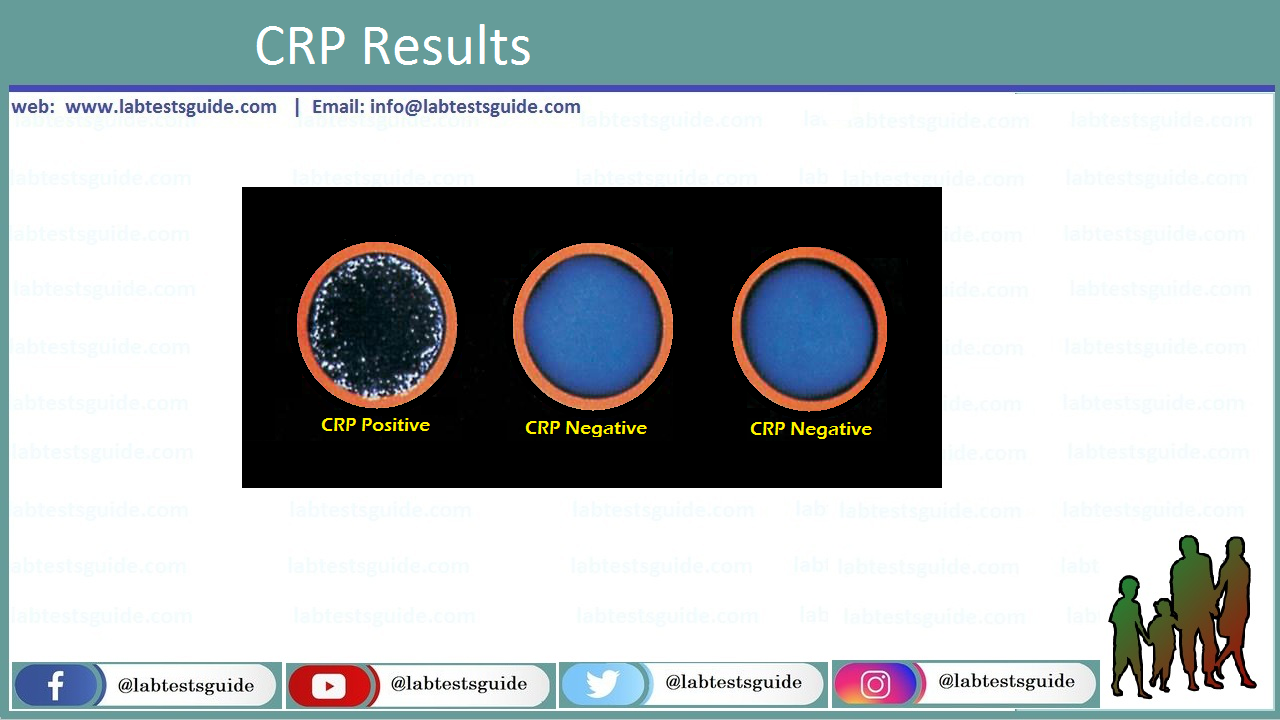
It is a slide agglutination test. Latex particles coated with CRP antiserum are allowed to react with test serum. Agglutination is observed if CRP is present in a concentration of 6 mg/L or above.
REQUIREMENTS:
- Serum sample
- CRP latex reagent
- Positive and negative controls (PC; NC)
- Test card and Test Tubes
- Normal saline
- Disposable mixing sticks
- Mechanical rotator (80-100 rpm)
PROCEDURE:
- Bring the kit reagents and sample to room temperature.
- Place 0.05 ml of the serum into one circle of slide.
- Place similar quantities of positive and negative controls in separate circles.
- Gently mix the latex reagent vial (to ensure homogeneity) and place one drop to each of the circle.
- Mix the contents of each circle evenly with disposable sticks and spread over the complete area of the circle.
- Place the slide on mechanical rotator (80-100 rpm) for 2 minutes.
- Examine for agglutination macroscopically.
- Compare the results with positive and negative controls.
RESULTS:
- Agglutination indicates a positive reaction.
- If CRP test is positive, the amount of CRP will be equal to 6 mg/L or above while in case of a negative reaction (no agglutination) less than 6 mg/L.
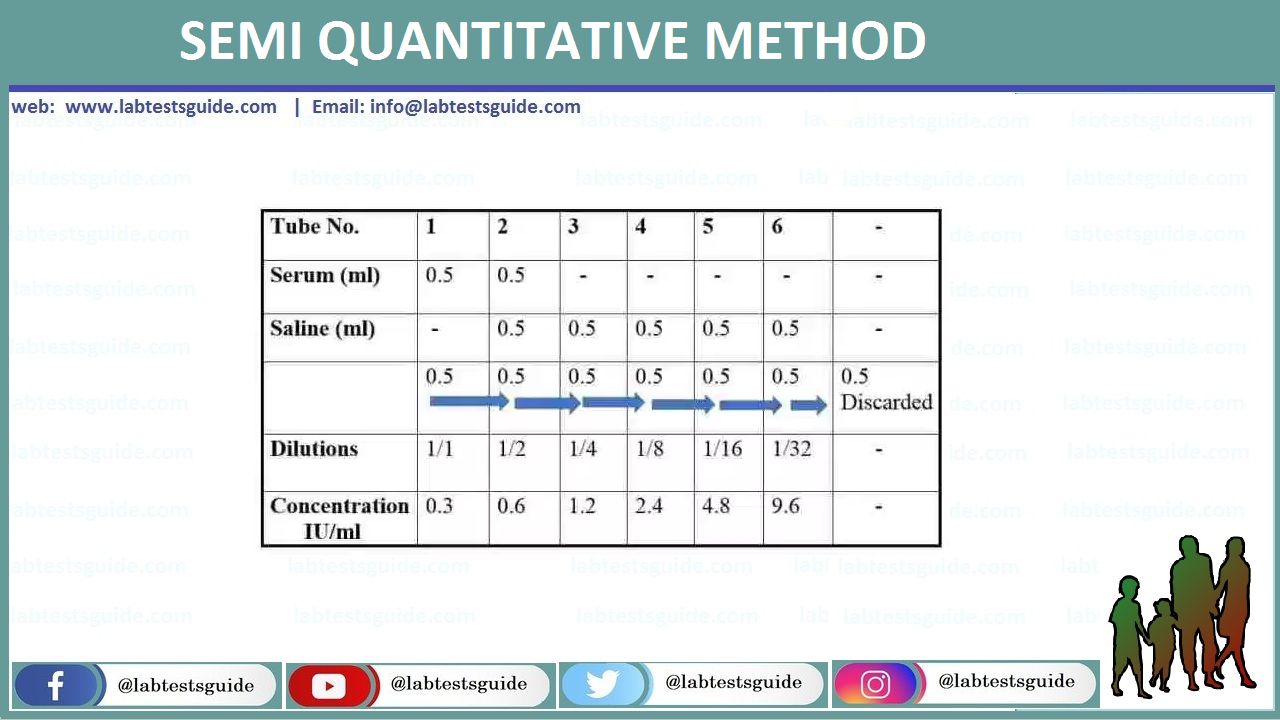
SEMI QUANTITATIVE METHOD:
- If CRP test is positive, serial dilutions of the serum are tested.
- The highest dilution of the serum giving positive result will be the titre.
Prepare double dilutions of serum as follows.
QUALITY CONTROL:
Every test kit have Positive and Negative controls which are run parallel to all tests which are being run or perform routinely.
INTERPRETATION OF CRP TEST:
- The increased level of CRP indicates inflammation and tissue damage.
- The progression of an infection is also monitored
- False negative results are seen due to prozone phenomenon.
- It is recommended to make the final diagnosis with clinical examination and other laboratory data.
COMPARISON OF CRP AND ESR TEST:
CRP has some advantages over Erythrocyte Sedimentation Rate (ESR), though both are used as a marker of inflammation.
- CRP is a direct measure of inflammation whereas ESR is a indirect one.
- CRP has a more rapid response to inflammation than ESR and also returns to normal when the inflammatory condition is resolved.
- CRP is comparatively less affected by age.
- CRP is not raised in non-inflammatory conditions but ESR is elevated in some.
Related Articles:
RELATED POSTS
View all